WHY DOES A CHILD NEED TUBES ?Indications for Ear Tubes
"Tubes", also called, "PE
Tubes", "PETs", or "Pressure Equalizing Tubes", allow
air to get into the middle ear space behind the eardrum. Air is needed in this space to allow the eardrum to move. Normally,
a tube (eustachian tube) at the
back of the throat does this, but in many children, the
eustachian tube
is immature or temporarily not fully grown, preventing the air from getting into
the middle ear. If
air is not present in the ear, either fluid builds up, or infections
start, or both. With the buildup of fluid or an infection, a
temporary or permanent hearing loss may develop. If a trial of
medication has not worked,
PE tubes may be recommended to prevent future problems. Prediction of which children
will develop complications from chronic serous otitis media is difficult. Measurement
of the ability to aerate the middle ear using the forced response test,
the sniff test and the pressure equilibration test has been found to be
of little value in the prediction of chronic serous otitis media
or the development of serious complications.
View AbstractClick on
Pictures to Enlarge
Another reason for the placement of ear tubes is
recurrent ear infections. Recurrent
middle ear
infections may be treated with
either long term antibiotics (prophylactic antibiotics) or ear tubes.
Because of developing bacterial resistance to antibiotics, many ear doctors are returning to
ear tube placement as one of the first line treatments for recurrent infection.
Does exposure to tobacco smoke cause ear infections ?
(Arch
OL-HNS July 1999)
View Abstract
To the right is a slide show of eardrums with chronic middle ear disease pre
and post ear tube (myringotomy tube) placement.
The eardrum on the promontory and the middle ear obliterated from adhesive otitis media.
There is scutal erosion with exposure of the head of the malleus and impending cholesteatoma formation.
The middle ear is filled with fluid and there is a shallow attic retraction pocket.
There is erosion of the long arm of the incus, an attic retraction pocket with exposure of the head of the malleus, & middle ear space obliteration.
There is a very deep retraction pocket with impending cholesteatoma formation.
Posterior retraction P\pocket with myringoincudopexy and impending cholesteatoma formation.
The eardrum has eroded the long arm of the incus and formed a myringostapediopexy.
This eardrum has a shallow attic retraction pocket.
This eardrum is retracted with mild tympanosclerosis. Note the thin area in the inferior eardrum from a prior tube placement.
This eardrum has severe tympanosclerosis with middle ear fluid and a myringoincudopexy.
This eardrum is retracted with tympanosclerosis and middle ear fluid. Note the severe scutal erosion and huge attic retraction pocket.
Ear (Myringotomy) Tube Surgery - Technique:
WHAT ABOUT COMING TO THE HOSPITAL?
Click on Pictures to Enlarge
It is VERY IMPORTANT on the day of surgery, that your
child have an empty stomach. If anything has been put into the mouth or
stomach, because of SAFETY for your child, the surgery must be
cancelled. Even chewing gum will cause the cancellation of surgery. DO
NOT let your child eat or drink ANYTHING on the day of surgery. Please
tell someone if you think your child has eaten or has drank anything on
the day of surgery. If there is food or liquid in the stomach at the
time of surgery, there is a chance your child could choke while asleep.
Search PubMed for Myringotomy Tubes
Laser assisted
myringotomy
for recurrent
acute otitis media
and chronic
serous otitis media
in children has been associated with a high
failure and persistence of the disease and with eardrum perforation.
View Abstract Koopman et..al. found that the eardrum
hole from a laser
myringotomy
stayed open an average of 2.4 weeks compared to 4 months for a
myringotomy
tube. The success rate for laser
myringotomy
was only 48% compared to 78% for
ear tube placement. Laser
myringotomy
was found to be safe but less effective than ear tube
placement. View Abstract
T-Tubes
are often called "permanent tubes". However, between 3.0% and 47%
(mean 8.8%) of T-Tubes will eventually come out (1). Kalcioglufound that T-Tubes will say in an average
of 16.3 months compared to 7.3 months for grommet tubes (2). When T-Tube
do come out they often leave a hole in the tympanic membrane. This is
significantly higher than the 0.5% to 2.0% perforation rate found in short-term
tubes (1) . Placing a T-Tube in a damaged eardrum or one that is markedly
retracted can produce perforation rates up to 21% (1).
(1)
Goode,
R.L. Long-term middle ear ventilation with T tubes: The
perforation problem. Otolaryngology-Head and Neck Surgery
1996;115:500-501.
(2) Kalcioglu MT, et.al. Follow-up of 366 ears after tympanostomy tube
insertion Otolaryngol Head Neck Surg 2003 Apr;128(4):560-4
View Abstractct
This picture to
the right shows a T-Tube coming out of the eardrum and a perforation forming
around the tube.
The picture to the right shows various
types of ear tubes.
Click on Pictures
to Enlarge
Ear (Myringotomy) Tubes - After The Surgery:
Will an ear tube need to be inserted if my
child's tube comes out ???
Click on Pictures
to Enlarge
The reinsertion rate for ear tubes is
between 15.9 % (Age over 18 months) to 26.3 % (age 18 months or
younger.) The greatest risk factor for reinsertion is a patient whose age is less than 18 months (3).
It is very important that your child has checkups every 3 to 6 months after the tubes are
put in so the tubes can be checked to determine it they are
still working.
The
picture to the right shows an ear tube which is starting to fall out of the
eardrum. The inner layers of the eardrum have healed behind the ear tube
and are pushing it off the eardrum. This usually takes place without
problems. However, sometimes a reaction occurs which produces excessive
serous fluid. When the fluid hardens in the center of the tube it is slowly
pushed out, causing the formation of a long rod shaped structure. The tube
shown in this picture was removed in the office without difficulty.
(3) Boston, M, McCook, J, and Derkay, C
Incidence of and risk factors for additional tympanostomy tube insertion in
children. Arch Otolaryngol Head and Neck Surg. 2003 Mar
129(3): 293-296.
View Abstract
HOW LONG WILL TUBES STAY IN?
Most tubes stay in place for 3 to 18 months,
average is 9 months, however, they can come out sooner or stay in longer.
However, this varies widely between patients. View
Article They usually come out on
their own and the drum usually heals. The first sign that the tube is coming
out is that it becomes plugged. This is caused by the eardrum healing
behind the tube. The tube will then be slowly pushed out.
Click on Pictures
to Enlarge
Can my child get water in his ears ???
Many
ENT Doctors feel that non-chlorinated water getting into the ear can cause
middle ear
infections. Because of this many ENT Doctors will recommend
wearing water ear plugs when bathing or swimming. In a recent article
Goldstein et. al. supports the use of water precautions in children who have
have had ear tube placement.
View
Article
Click on Pictures to
Enlarge
Ear (Myringotomy) Tube Surgery -
Complications:
Sometimes bleeding occurs when the
tubes are coming out. The use of ear drops usually stops the bleeding and
allows the tubes to come out naturally. If the tubes stay in for 3 years your
doctor may want to remove them by taking your child back to the operating room.
Rarely (1%), a hole is left in the eardrum when the tubes come out. This
hole will act as a tube, but at some point the child will have to be taken back
to the operating room and have the hole patched. This procedure may be
postponed until the child is 6 to 8 years of age.
It is very important that your child has checkups every 3 to 6 months after the tubes are
put in so the tubes can be checked to determine it they are
still working.
When
tubes stop working it is usually because they have become plugged or the
eardrum has healed behind the tube. If the ear tube is plugged it
often can be unplugged in the office. However, if the eardrum has
healed behind the tube and the tube is still needed, then tube reinsertion
may have to be performed.
This
picture shows an ear tube with pus draining out of it in a child with an
acute otitis media
(middle ear
infection).
Up to one
third of infections in ears with ear tubes is due to a bacteria called
pseudomonas. This bacteria is resistant to almost all oral antibiotics
which can be given to children. If ear drops do not clear the infection, the
child may rarely have to be placed on IV medications through home health.
Treatment with ear drops containing neomycin have the potential for
ototoxicity,
but have been used for many years with few adverse effects.
View Abstract A new
generation of ear drops which contain fluoroquinolone antibiotics ( cipro and
floxin ear drops ) are also effective against pseudomonas and are not
ototoxic.
View Abstract
Heslop et. al reported that topical ciprofloxacin had a 23% failure rate which
was lower than that found in patients treated with oral amoxicillin or with
saline rinses.
View Abstract
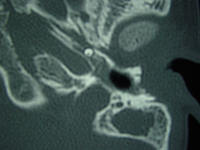
Rarely
an ear tube does not fall out into the ear canal but instead falls into the
middle ear.
Usually, this does not cause a problem and the tube does not have to be removed.
The two pictures on the right shows ear tubes which
have migrated into the middle ear.
Click on Pictures to
Enlarge
This
picture shows an infected ear tube with pus draining out of the tube and an
infectious granuloma
above the ear tube.
Click on Pictures to
Enlarge
This
picture is of a 12 year old who had ear tubes placed six years ago.
Granulation tissue
has completely grown over and enveloped the tube.
The ear had chronic drainage from the
granulation tissue.
The eardrum was mobile and the ear tube was plugged with tissue.
Surgical tube removal will probably be required.
Click on Pictures to
Enlarge
The
picture on the right shows a picture of an ear with an
acute otitis media
(
middle ear
infection ) with an extruded ear tube, laying in the ear canal.
The picture on the left shows a perforation and a
granulomawhich formed from an ear tube
The
picture on the far right shows a perforation from a
myringotomy tube.
The near right picture shows an inferior
perforation with an anterior area of tympanosclerosis and an extruded ear tube
in the superior ear canal. Eardrum perforations occur in about 2% of ears.
View Abstract
Click on Pictures to
Enlarge
cholesteatoma
is a rare complication of myringotomy tube
placement, but can occur. To the right is a picture of a child two years
after myringotomy tube placement. A white round
cholesteatoma
can be seen in the area where the tube resided.
This
picture shows an eardrum with
tympanosclerosis
or white plaques of the eardrum which form from
prior infections.
The plaques are surrounding a "monolayer" or thin portion of the
eardrum. Not how through the hand held
otoscope
the monolayer mimics a perforation but the close up
view clearly shows the intact eardrum. A monolayer is sometimes occurs
when an eardrum perforation heals. In this patient the monolayer formed
after an ear tube extruded.
Click on
Pictures to Enlarge
The
picture to the right shows an 80 year old patient had a
nasopharyngeal(back of the nose) mass which presented with blockage of the
eustachian tube
and
serous otitis media
( ear fluid ). The mass was a
benign
cyst (Tornwaldt's Cyst) but could have been
a cancer. Older patients that present with persistent ear fluid should
have an examination of the
nasopharynx.
Google Ad space finances and sponsors
ENT USAtm Websites. ENT USAtm,
Cumberland Otolaryngology or Dr Kevin Kavanagh, MD do not endorse,
recommend, referrer to or are responsible for the Advertisements or
for the content or claims made in the Advertisements.









 The eardrum on the promontory and the middle ear obliterated from adhesive otitis media.
The eardrum on the promontory and the middle ear obliterated from adhesive otitis media.


 There is scutal erosion with exposure of the head of the malleus and impending cholesteatoma formation.
There is scutal erosion with exposure of the head of the malleus and impending cholesteatoma formation.
 The middle ear is filled with fluid and there is a shallow attic retraction pocket.
The middle ear is filled with fluid and there is a shallow attic retraction pocket.
 There is erosion of the long arm of the incus, an attic retraction pocket with exposure of the head of the malleus, & middle ear space obliteration.
There is erosion of the long arm of the incus, an attic retraction pocket with exposure of the head of the malleus, & middle ear space obliteration.
 There is a very deep retraction pocket with impending cholesteatoma formation.
There is a very deep retraction pocket with impending cholesteatoma formation.
 Posterior retraction P\pocket with myringoincudopexy and impending cholesteatoma formation.
Posterior retraction P\pocket with myringoincudopexy and impending cholesteatoma formation.


 The eardrum has eroded the long arm of the incus and formed a myringostapediopexy.
The eardrum has eroded the long arm of the incus and formed a myringostapediopexy.
 This eardrum has a shallow attic retraction pocket.
This eardrum has a shallow attic retraction pocket.
 This eardrum is retracted with mild tympanosclerosis. Note the thin area in the inferior eardrum from a prior tube placement.
This eardrum is retracted with mild tympanosclerosis. Note the thin area in the inferior eardrum from a prior tube placement. 
 This eardrum has severe tympanosclerosis with middle ear fluid and a myringoincudopexy.
This eardrum has severe tympanosclerosis with middle ear fluid and a myringoincudopexy.


 This eardrum is retracted with tympanosclerosis and middle ear fluid. Note the severe scutal erosion and huge attic retraction pocket.
This eardrum is retracted with tympanosclerosis and middle ear fluid. Note the severe scutal erosion and huge attic retraction pocket.